
Drugs and Harm in the UK: Researching the Association
Table of Contents
Introduction
Drugs and harm in the UK has become a central political issue. Drugs such as alcohol and tobacco products are a major cause of harm to individuals and society. They are regulated by taxation, sales, and restrictions on the age of purchase. Concern about drugs and the harm they cause in the UK has led to stiffening laws and reduced availability across the territory. Drug policy should be shaped by a clear understanding of the harms those substances create, and this study sought to do exactly that.
Evaluation Criteria for a Drug’s Harm
There are many factors that contribute to a drug’s overall harm profile. Experts were asked to score each drug according to nine criteria, from the intrinsic harms of the drugs to their downstream social and healthcare costs. Drug harms were then reviewed by experts to create a model with the multicriteria decision analysis (MCDA) approach. This approach structures and evaluates multiple conflicting criteria in order to lead to more informed decisions.
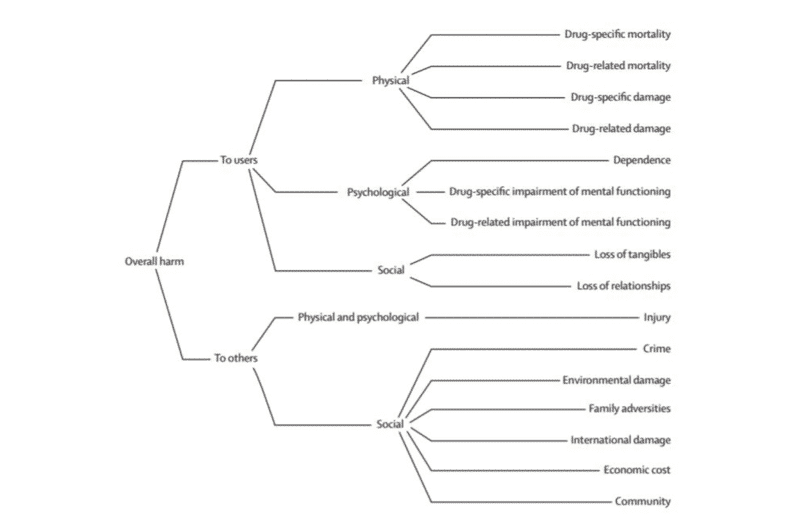
The MCDA yielded 16 harm criteria (see below for definitions). Nine relate to harm of the individual or user, and seven to the harm of others. These criteria were then clustered into five subgroups representing physical, psychological, and social harms (see figure 1).
In June 2010, a meeting supported by the Independent Scientific Committee on Drugs (ISCD), a non-governmental expert organization, further developed the MCDA model. They sought to generate scores for 20 different drugs that are relevant to the UK, spanning a range of potential harms. Harm criteria were scored and the relative importance of each criterion was assessed. This method resulted in a common unit of harm across all the criteria, from which a new analysis of relative drug harms was achieved.
Drugs and Harm: Criteria and Definitions
- Drug-specific mortality: How lethal is the drug to an adult, relatively speaking
- Drug-related mortality: The extent to which life is shortened by the use of the drug, such as from vehicle accidents, lung cancers, HIV, suicide, etc.
- Drug-specific damage: Damage to physical health drawn directly from the drug, such as from cirrhosis, seizures, strokes, stomach ulcers
- Drug-related damage: Damage to physical health as a consequence the drug, such as unwanted sexual activities, blood-borne viruses, emphysema, and self-harm
- Dependence: The extent to which a drug creates a propensity to continue to use it despite adverse consequences
- Drug-specific impairment of mental functioning: For example, amphetamine-induced psychosis, ketamine intoxication
- Drug-related impairment of mental functioning: For example, mood swings or depression
- Loss of tangibles: Does consumption lead to the loss of income, housing, a job, imprisonment
- Loss of relationships: Does it lead to a loss of relationship with family and friends
- Injury: Does the drug increase the chance of injuries to others, if from violence, vehicle accidents, or fetal harm
- Crime: Extent to which the use of a drug leads to an increase in crime
- Environmental damage: Does the drug damage the environment, as in toxic waste from amphetamine factories or discarded needles
- Family adversities: Does the drug drive a breakdown in the function of the family, from economic loss, emotional wellbeing, or a child’s future prospects
- International damage: Does the use of drugs in the UK contribute to international harm, such as deforestation or international crime
- Economic cost: Does the drug directly drive costs within the UK, as in health care costs, policing, prisons, rehabilitation services, or insurance claims
- Community: Does the drug drive a decline in social cohesion or reputation of the community
Drugs were scored with points out of 100.
The Association Between Drugs and Harm in the UK: Study Results
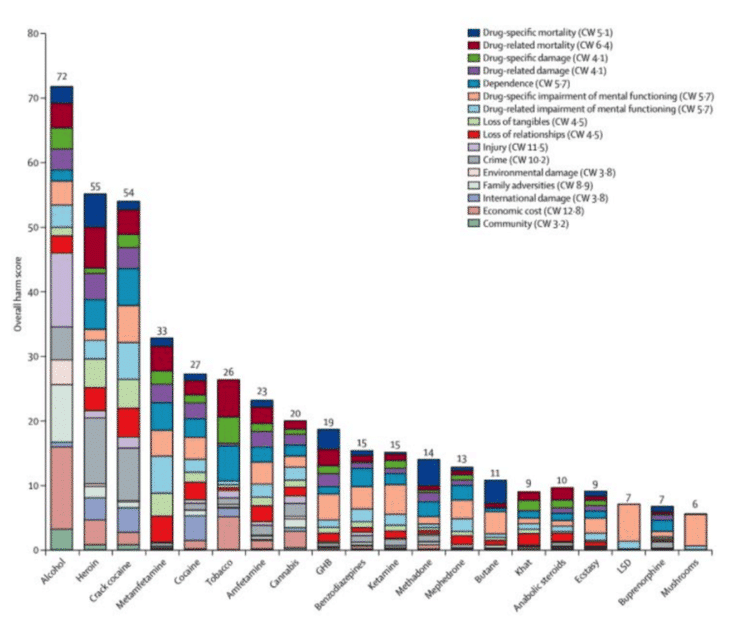
The results above show the harms of a range of drugs in the UK. Alcohol had the highest overall harm score in the study, at 72, while psilocybin finished with the LOWEST score, of 5. Alcohol scored fourth on harms to users and top for harms to society. Regarding only the toxic effects, alcohol is also more lethal than many illicit drugs, such as cannabis, lysergic acid diethylamide (LSD), or magic mushrooms.
Social harms are harder to measure. Estimates from vehicle and at-home accidents, drug-related violence, and the costs to economies in provider countries (Colombia, Afghanistan, Mexico) give some guidance, and largely reflect those of the more direct harms.
A low score in this assessment doesn’t necessarily mean the drug is not harmful, since all drugs can be harmful under specific circumstances. However, it’s clear that official legislation in the UK places some of the greatest weights against the least harmful substances. A subsequent study was performed that sought the correlation between the actual harm caused by a drug (from this study), and the severity of that drug’s classification in the UK’s ‘Misuse of Drugs Act‘. The correlation between the harm caused by a drug and its severity in the Act is 0.04. This effectively means no correlation at all. Essentially, UK drug and harm reduction policy is much too lenient on some substances, and much too hard on others. It’s quite clear that alcohol is, by a good margin, the most dangerous drug available in the UK.
Epilogue
Perhaps the most interesting part of the research into Drugs and Harm in the UK happened after it was published. The study’s Lead Investigator, the former Chief Drug Advisor to the UK Government, David Nutt, was asked to resign as Chair of the Advisory Council on the Misuse of Drugs. The former Home Secretary took issue with the study’s assertion that MDMA and LSD were less dangerous than alcohol or tobacco. The dismissal definitely raised eyebrows and brought into question the Home Secretary’s motivations. Richard Garside, Director of the Centre for Crime and Justice, said Nutt’s paper gave an insight into what drug policy might look like if it was based on the research evidence rather than political or moral positioning. He also added “the Home Secretary’s action is a bad day for science and a bad day for the cause of evidence-informed policy making.” Drug policy and lawmakers need to align themselves with science, data, and the betterment of public health overall.
This article is part of Frshmind’s “Psychedelic Science Snapshot Series” where Frshminds reviews the latest in psychedelic research.
Comments